
Healthcare accounts receivable management in behavioral health depends on clean claim submission, payer-specific follow-up, and documentation practices that support timely appeals. When any of these breaks down, cash slows and write-offs climb. Your A/R performance is a direct readout of how well your clinical, billing, and operations functions are working together.
Key Takeaways
- Clean claims rate above 95% is the operational target; most behavioral health programs start in the mid-80s and improve with focused fixes to intake data quality and authorization workflows.
- Industry benchmark for days in A/R is fewer than 40 days; high-performing organizations often reach 30–35 days through proactive denial management and payer-specific follow-up.
- Denial escalation follows a tiered timeline, primary follow-up at 15–30 days, secondary at 30–45 days after adjudication, internal patient collections at 60–90 days.
A/R KPI Reference for Behavioral Health
These are some of the best healthcare accounts receivable management KPIs that you should be tracking.
| Metric | Definition | Behavioral Health Target | Why It Matters |
| Net Collection Rate | Cash collected ÷ (charges − contractual adjustments) | 95%+ for commercial; lower for Medicaid-heavy mix | Summarizes coding, submission, payer execution, and patient collections in one number |
| Days in A/R (DSO) | Average days claims remain outstanding | <40 days; high performers: 30–35 days | Persistent >60 days signals systematic billing or follow-up failures |
| Clean Claims Rate | Claims accepted on first submission ÷ total claims | 95%+ | Directly reduces rework cost and accelerates cash |
| Denial Rate | Claims denied ÷ total claims submitted | <5% | Higher rates indicate upstream intake or coding failures |
| Patient Collections Rate | Patient cash collected ÷ patient balances billed | Varies by self-pay mix; track trend monthly | High deductible plan growth makes this increasingly material |
| 90+ Day A/R Bucket | Balance aged >90 days ÷ total A/R | <15–20% | Anything higher suggests claims are aging past appeal windows |
Healthcare Accounts Receivable Management Key Performance Indicators and Why They Matter
Behavioral health operators benefit from tracking a concise set of KPIs that directly reflect cash flow, process quality, and operational risk. Chasing too many healthcare accounts receivable management metrics dilutes focus; the six measures above give revenue leaders a reliable picture of where the cycle is healthy and where it is straining.
Tracking these KPIs consistently also feeds the reporting and predictive models described later in this guide.
Focusing on these measures helps your team prioritize workflow improvements that reduce administrative burden while improving both cash flow and patient experience with billing. Track each KPI by payer segment, not just in aggregate.
A facility can post a healthy 28-day average with commercial carriers while carrying a problematic 65-day average with a Medicaid managed care plan, a distinction that disappears in aggregate healthcare accounts receivable management reporting.
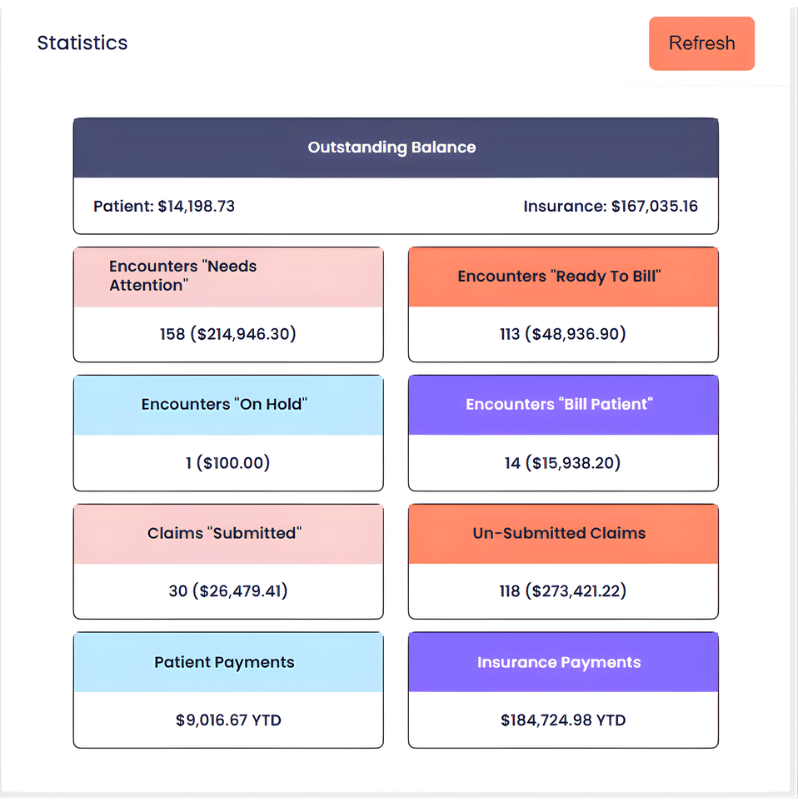
Here’s an example of a healthcare accounts receivable management tracking dashboard in Alleva, which can help see outstanding bills at a glance:
How to Calculate Net Collection Rate
Net collection rate for healthcare accounts receivable management measures how effectively your organization converts allowed charges into cash. The formula:
Net collection rate = (Total cash collections ÷ [Total charges − Contractual adjustments]) × 100
Use the same period for collections and charges to avoid timing distortion. Exclude reverse payments and non-operational receipts for clarity. Benchmarks vary by payer mix, behavioral health programs with high Medicaid and state contract exposure will typically track lower net collection rates than largely commercial practices, which is a structural reality rather than a performance failure.
Improving net collection rate often means fewer denials, faster cash, and lower collection costs. It captures coding accuracy, claims submission quality, payer contract execution, and patient collections in one healthcare accounts receivable management metric that is easy to communicate to leadership and boards.
Healthcare Accounts Receivable Management Pro Tip #1
Track your net collection rate by payer segment, not just in aggregate. A blended rate can mask a high-performing commercial book subsidizing poor Medicaid or managed care performance—or vice versa. Segmenting by payer class surfaces where denials, underpayments, or write-off patterns are actually eroding revenue, so your team can prioritize the right interventions rather than chasing an average.
What Is a Clean Claim and How Is Clean Claims Rate Measured
A clean claim contains complete and accurate patient demographic and insurance information, valid provider identifiers, correct CPT/HCPCS and ICD coding, appropriate modifiers, and service dates that match documentation. It also includes required prior authorizations and carries no obvious administrative errors that would trigger an automatic rejection.
Clean claims rate = (Claims accepted for adjudication without manual correction or denial on first submission) ÷ (Total claims submitted) × 100
A healthcare accounts receivable management rate above 95% is a strong operational target; many behavioral health programs start in the mid-80s and improve through focused interventions. Track by payer and service line to prioritize root cause fixes, intake data quality, authorization workflows, and coder training are the most common leverage points.
A/R Aging Benchmarks and Dollar-Weighted Payer Analysis
These are some healthcare accounts receivable management benchmarks you can use to establish your own goals:
| Aging Bucket | Action Standard | Risk Signal |
| 0–30 days | Normal adjudication window; monitor only | No action required if clean claim rate is >90% |
| 31–60 days | Begin active follow-up; verify submission and receipt | Check for timely filing exposure on complex claims |
| 61–90 days | Escalate to dedicated A/R specialist; document all contacts | Likely denial, authorization gap, or duplicate issue |
| 91–120 days | Priority appeals; clinical review for medical necessity denials | Risk of timely filing window closure |
| 120+ days | Evaluate for write-off, secondary payer, or patient escalation | High write-off risk; root cause investigation required |
| Patient balances 60–90 days | Internal collections outreach; financial counseling referral | High-deductible plans increase patient balance exposure |
Tracking A/R separately by payer is essential for accurate diagnosis and continued healthcare accounts receivable management optimization. Medicaid programs often have longer adjudication timelines than commercial carriers, and state-specific billing requirements add friction that aggregate reporting obscures.
Your billing and RCM workflows should surface payer-level aging automatically rather than requiring manual segmentation.
Denial Prevention, Categorization, and Escalation Workflows
Denial management performs best when it is designed around prevention first, then quick triage, then prioritized appeals. Prevent denials by standardizing intake fields, verifying eligibility and benefits before service, requiring prior authorization where needed, and validating provider credentials before submission. Your verification of benefits process is the upstream gate that shapes how your A/R behaves downstream.
Triage by classifying denials into categories: eligibility, coding, medical necessity, duplicate, timely filing, or coordination of benefits. Route each category to a specialized owner — eligibility issues to intake, coding denials to documentation and coding teams, medical necessity denials to clinical review and appeals.
Behavioral health organizations billing under 42 CFR Part 2 face additional documentation constraints that make proactive authorization tracking especially important.
A reliable healthcare accounts receivable management denial workflow reduces rework and preserves clinical time by focusing administrative effort where it yields the largest return. Appeal clinical denials quickly with supporting documentation, and prioritize high-dollar and high-probability claims to protect cash within timely filing windows.
Healthcare Accounts Receivable Management Pro Tip #2
Build a denial reason code library mapped to root causes and fix owners before you build anything else. Most denial categories trace back to a small number of repeating process failures, the same intake field left blank, the same authorization step skipped, the same payer-specific rule missed.
When every denial is coded to a root cause and assigned to a process owner, your monthly denial review shifts from reviewing symptoms to closing loops. Patterns become visible in weeks rather than quarters, and your prevention efforts compound over time instead of resetting with every new staff cycle.
How Long Before Escalating Unpaid Claims
For primary payer follow-up, begin continuous monitoring with a documented check at 15–30 days if no response after submission. Secondary payer follow-up begins 30–45 days after primary adjudication or when a primary denial signals secondary responsibility.
Internal patient collections outreach typically starts 60–90 days past the patient statement, with formal external collections considered after 90–120 days, subject to state law, internal charity policy, and balance size.
High-dollar or high-complexity claims warrant earlier escalation to stay within appeal windows. When a patient is on an income-based assistance plan or has an active Good Faith Estimate dispute, delay or modify collections in accordance with your financial assistance policy. These timeframes balance administrative efficiency, payer appeal rights, and patient experience.
Documentation to Retain for Appeals
Maintaining organized, retrievable healthcare accounts receivable management documentation is the foundation of a strong appeals practice. Retain intake and demographic forms, signed consents and treatment agreements, prior authorization logs, progress notes and treatment plans, discharge summaries, and billing records.
Also keep original claims, corrected claims, EOBs, and complete payer communication logs with dates, contacts, and outcomes. Your compliance documentation systems should make these records retrievable on short notice, for payer appeals, audits, and accreditation reviews alike.
A consistent tagging and indexing system reduces time to assemble appeals and increases success rates for any area of healthcare accounts receivable management. Behavioral health organizations with high medical necessity denial rates often find the root cause in clinical documentation, not billing, which makes progress note quality and treatment plan specificity as much a revenue issue as a compliance one.
How Payer Mix Affects A/R Performance
Payer mix shapes reimbursement levels, denial profiles, and payment timing in ways that materially change how your A/R team needs to operate. Higher Medicaid or state-contracted volume typically reduces allowable reimbursement rates and increases administrative complexity through state reporting requirements and longer adjudication timelines.
Commercial and managed care payers often pay higher rates but require strict credentialing, complex contract terms, and more rigorous prior authorization.
Self-pay and uninsured volumes increase patient collections work and financial assistance needs, a growing challenge as high-deductible health plan adoption continues to shift more cost responsibility to patients. Segment your A/R reporting by payer class and build payer-specific playbooks: faster appeals for commercial denials, compliance checklists for state payers, and financial counseling programs for self-pay populations.
Adjust cash reserves and forecasting assumptions to reflect payer-specific payment timing and denial rates, so your leadership team is not surprised by temporary dips when a payer changes its adjudication cycle.
Staffing Ratios for an A/R Follow-Up Team
Staffing ratios for healthcare accounts receivable management depend on automation level, payer mix complexity, and the proportion of self-pay in your patient population. The ranges below are directional starting points, reassessed regularly using productivity metrics like A/R touches per FTE and dollars collected per FTE.
| Revenue Tier | A/R Follow-Up FTEs | Patient Collections FTEs | Notes |
| Under $2M | 0.5–1 specialist (shared) | Shared with billing | Often combined with biller role |
| $2M–$5M | 1 specialist + shared manager | 0.5–1 FTE | Add collections resource as self-pay grows |
| $5M–$10M | 2–3 FTEs | 1–2 FTEs | Dedicated payer follow-up lanes recommended |
| $10M–$25M | 4–6 FTEs | 2–3 FTEs | Add appeals specialist for medical necessity |
| $25M+ | 1 FTE per $2M–$4M revenue | 1 FTE per $3M–$5M patient liability | Add dedicated reporting and supervisory roles |
Typical roles at scale include A/R follow-up specialists, patient collections specialists or financial counselors, an appeals/clinical review specialist for medical necessity work, and an RCM manager or supervisor. Healthcare accounts receivable management automation, particularly for eligibility verification and remittance posting, can extend the effective range of each FTE.
Estimating the Financial Impact of Reducing Days in A/R
To estimate the working capital impact of reducing days in A/R, divide annual net revenue by 365 to get average daily revenue, then multiply by the number of days you want to reduce.
For an organization with $12M in annual revenue, average daily revenue is approximately $32,877. Reducing days in A/R by 10 days frees roughly $328,767 in working capital, a meaningful liquidity gain from operational discipline alone.
Factor in collection costs and potential changes to write-offs when modeling the net benefit. The calculation assumes collections speed increases uniformly, while real results depend on payer behavior and patient payment patterns. Leaders can use the model as a quick order-of-magnitude check before committing to workflow changes or staffing investments in their healthcare accounts receivable management systems.
AI-Assisted A/R Prioritization: A 2025–2026 Development
A growing number of behavioral health billing platforms now embed predictive A/R tools that use historical claims data to generate claim-aging risk scores and route follow-up work automatically. Rather than working an aging report in calendar order, your healthcare accounts receivable management team follows a prioritized queue where high-dollar, high-probability claims surface first.
Denial propensity modeling, identifying which claims are statistically likely to be denied based on payer, diagnosis, and service type, allows proactive correction before submission rather than reactive rework after rejection.
Remittance pattern analysis, drawing on 835 electronic remittance advice transactions, adds another layer. Systematic healthcare accounts receivable management analysis of remittance data by payer can reveal patterns, such as a carrier consistently reducing allowed amounts for a specific behavioral health service, that directly affect A/R resolution timelines and contract negotiation leverage.
Automated appeals routing uses the specific denial reason code and payer guidelines to generate appeals documentation with minimal manual effort across the healthcare accounts receivable management process.
Your EMR and billing platform choice directly determines whether these capabilities are available to your team. An all-in-one behavioral health platform that connects clinical documentation, claims generation, and A/R management in a single system is better positioned to support this kind of intelligence than a collection of disconnected point solutions.
Healthcare Accounts Receivable Management Pro Tip #3
Before evaluating AI-assisted A/R tools, audit the quality of your historical claims data first. Predictive models are only as accurate as the data they train on. If your legacy system has inconsistent denial coding, incomplete remittance matching, or gaps in payer-level documentation, the risk scores and propensity models built on that data will inherit those blind spots.
Clean, consistently coded data over 12 to 24 months is the foundation that separates genuinely useful A/R intelligence from a prioritization queue that just repackages your existing workflow. Ask vendors how their models were trained, on what payer mix, and whether behavioral health claim types are represented.
Generic revenue cycle models built predominantly on medical-surgical data may not reflect the authorization patterns, diagnosis coding conventions, or payer behavior specific to behavioral health billing.
Minimum Data Elements for Predictive A/R Models
Effective predictive prioritization requires structured data at the claim level, submission date, claim ID, billed and allowed amounts, claim status, denial codes, and payment amount.
Pair that with patient demographics and guarantor data, payer plan type and historical payment lag, clinical metadata, provider identifiers, interaction history, and contractual rates where available.
With these healthcare accounts receivable management elements, a model can prioritize claims by estimated collectability, days to expected payment, or likelihood of successful appeal. The data also supports proactive intervention, flagging claims approaching timely filing deadlines before they become unrecoverable.
Business Intelligence and Reporting for Behavioral Health A/R
Design reports for role-specific decisions rather than generic aging summaries. Executive dashboards should surface net collection rate, days in A/R, top payer aging, and cash receipts trends.
Healthcare accounts receivable management operation views should show claims aging buckets, denial reasons by volume and payer, and active triage queues. Collections and patient-facing reports should track statement aging, promise-to-pay status, and financial assistance pipeline volume.
Reports are only useful when they are actionable, updated with trustworthy data, and tied to named owners for each KPI. Clear reporting reduces repeated manual audits and supports the continuous improvement cycle that moves your A/R performance from reactive to proactive.
Many behavioral health organizations also find that strong reporting becomes a compliance asset, providing documentation trails for payer audits and accreditation reviews.
Aligning Financial Policies with the No Surprises Act and Good Faith Estimates
Behavioral health organizations serving uninsured or self-pay patients should review their financial policies and patient statements for alignment with No Surprises Act requirements. Publish and make accessible a Good Faith Estimate policy that describes how GFEs are created, what triggers them, and how patients can request them.
Train intake and financial counseling teams to deliver GFEs to uninsured or self-pay patients within the statutory timeframe and to document delivery systematically.
Update patient-facing statements to include required notices and dispute resolution contact information where applicable. Review your financial assistance, collections, and billing timelines to confirm they do not conflict with GFE dispute rights or protection windows.
Maintain records of disclosures and patient acknowledgments for audit support, the same documentation discipline that strengthens your payer appeals practice also protects your organization from regulatory exposure.
Schedule a Demo to See Alleva’s Billing and A/R Tools
If your behavioral health organization is managing aging claims, denial backlogs, limited payer visibility, or disconnected billing and clinical documentation, explore whether Alleva’s all-in-one platform can support a more connected revenue cycle.
Alleva is designed to help behavioral health teams submit cleaner claims, follow up with more precision, and maintain the compliance documentation that supports faster appeals.
Schedule a demo to see how workflow-driven documentation, payer-aware RCM tools, and built-in reporting can work together for your organization.
Frequently Asked Questions: Healthcare Accounts Receivable Management
How do you calculate net collection rate for a behavioral health practice?
Net collection rate equals total cash collections during a period divided by charges for the same period minus contractual adjustments, expressed as a percentage. It summarizes how effectively your organization converts billed services into cash after payer contracts and write-offs, reflecting coding quality, submission accuracy, payer execution, and patient collections in a single metric.
What is a clean claim and how is clean claims rate measured in practice?
A clean claim has complete patient and insurance information, correct provider IDs, appropriate codes and modifiers, matching service dates and documentation, and required prior authorizations. Clean claims rate is the number of claims accepted without manual correction or denial on first submission divided by total claims submitted.
Tracking by payer and service line helps focus improvements where they will have the largest impact on rework reduction.
How long should a behavioral health provider wait before escalating an unpaid claim?
Begin secondary follow-up about 30–45 days after primary adjudication or when a primary denial signals secondary responsibility. Start internal patient collections outreach around 60–90 days after statement issuance, and consider external collections after 90–120 days subject to state law, financial assistance policies, and the patient situation. High-dollar or time-sensitive claims require earlier escalation to stay within appeal windows.
What documentation should be retained to support appeals and prevent repeated denials?
Retain intake and demographic records, signed consents, prior authorizations, progress notes and treatment plans, discharge summaries, billing records, original claims, corrected claims, EOBs, and payer communication logs. Tagging and indexing these for quick retrieval shortens appeal turnaround and reduces the likelihood of repeated denials on the same claim type.
How does payer mix affect A/R performance and what operational adjustments help?
Payer mix affects reimbursement levels, denial profiles, and payment timing. Medicaid-heavy mixes often bring lower reimbursements and longer adjudication timelines, while commercial mixes typically yield higher rates but stricter credentialing requirements. Segment your A/R by payer, create payer-specific playbooks, adjust staffing and automation accordingly, and build cash-flow reserves consistent with your specific mix.
What staffing ratios apply to an A/R follow-up team by revenue volume?
Staffing ranges vary by automation and complexity, but directional guidelines are: under $5M revenue, one A/R specialist plus a shared manager; $5M–$25M, roughly one A/R FTE per $1.5M–$3M of annual revenue plus patient collections coverage; above $25M, approximately one FTE per $2M–$4M with dedicated appeals and supervisory roles. Reassess regularly using productivity metrics.
How can organizations estimate the financial impact of reducing days in A/R by 10 days?
Divide annual net revenue by 365 to get average daily revenue, then multiply by 10. A $12M-revenue organization would free approximately $328,000 in working capital from a 10-day reduction. Adjust for realistic collectability and incremental collection costs to model the net benefit accurately.
What minimum data elements are needed to run predictive A/R prioritization models?
Key elements include claim-level fields (submission date, status, billed and allowed amounts, denial codes), patient demographics and guarantor data, payer identifiers and plan type, clinical metadata such as diagnosis and service type, provider IDs, interaction history, and contractual rate data where available. These fields support models that estimate likelihood of payment and prioritize high-value follow-up.
How should providers update financial policies to comply with No Surprises Act and GFE requirements?
Document how GFEs are produced and delivered, train staff to provide them to uninsured or self-pay patients within required timelines, and update patient statements to include required notices and dispute resolution contacts. Ensure collections timelines respect dispute rights and maintain disclosure records for compliance verification.