EHR billing in behavioral health connects clinical documentation to payer submission so that admissions, treatment notes, and group sessions flow into clean claims without re-keying. Healthcare organizations running mental health and addiction programs increasingly expect their EHR systems to absorb this billing workflow rather than handing it off to a separate platform.
This guide explains how integrated revenue cycle management (RCM) works inside a behavioral health Electronic Health Record (EHR) platform, how to evaluate vendors, and how to track whether yours is moving the needle on cash flow and denials.
If you operate a substance use disorder (SUD) or mental health program (outpatient, intensive outpatient (IOP), partial hospitalization (PHP), residential, or detox) the EHR billing rules are not the same as a primary care or hospital setting.
At Alleva, we built our platform specifically for behavioral health, which is why we wrote this guide around the workflows your team actually runs.
Key Takeaways
- Level of care drives the billing model: Detox and residential typically bill per-diem (H0010, H0017, H0018); PHP and IOP often blend per-diem and per-encounter; outpatient therapy bills per-session (90834, 90837); MAT can be bundled or unbundled depending on payer.
- Track six core KPIs: Clean-claim rate (target 90–95%+), first-pass acceptance (95%+), days in A/R (under 40), denial rate (under 5–7%), net collection rate (95%+), and admission-to-billing lag (under 72 hours).
- The new layer is AI-powered prior authorization and appeals: Electronic prior authorization (ePA) using HL7 DaVinci PAS and FHIR, plus generative-AI appeal drafting, are reshaping behavioral health revenue cycle in 2024–2026.
Want to see what integrated EHR + RCM looks like for a behavioral health program? Request a demo.
What EHR Billing Means for Behavioral Health Operators
EHR billing converts clinical documentation into billable claims. The system maps therapy notes, treatment plans, assessments, medication orders, and group attendance to charge capture, coding, claim assembly, and electronic submission, without forcing your EHR billing team to re-enter data the clinical team already documented in the patient record.
For behavioral health, the workflow runs from admission and verification of benefits (VOB), including a structured medical history review, through clinical documentation, charge capture, coding, scrubbing, submission, remittance posting, and denial follow-up. Each handoff is a potential revenue leak. A connected workflow tightens those handoffs into a single chain of custody for the encounter data.
Claims are commonly transmitted as CMS-1500 (professional) or UB-04 (institutional) forms. They route through a clearinghouse using X12 837 transactions, and remittances come back as X12 835. The CMS administrative simplification standards define these formats and the rules around them.
Benefits of Connecting Clinical and Billing Workflows
Integrated EHR and billing workflows reduce duplicate data entry, accelerate submission, and produce audit-ready trails, three outcomes that matter as much for compliance posture as they do for cash flow. When charges post automatically from documented encounters and progress notes, transcription errors fall and clean-claim rates can rise.
Linking patient charts directly to charge capture also helps EHR billing codes match documented care. That alignment is what insurance payers look for during audits, and it reduces the number of “documentation does not support billed level” denials that consume so much rework time.
For behavioral health programs, this matters most across admissions-to-treatment billing, group therapy splits, MAT, and telehealth modifiers. A connected platform likeAlleva’s behavioral health EMR can support faster adjudication and more accurate revenue forecasting when configured to your payer mix.
Behavioral Health Billing Workflows by Level of Care
Behavioral health does not bill the same way at every level of care. The unit of EHR billing, the documentation cadence, and the code set shift as the program intensity changes, and getting this mapping right is one of the highest-leverage configuration decisions you make at implementation.
The table below summarizes the most common patterns. Payer-specific contracts and state Medicaid plans will modify these, so treat the table as a starting frame rather than a final specification.
Behavioral Health Levels of Care and EHR Billing Patterns: Simple Chart
| Level of Care | Common Billing Unit | Representative Codes | Documentation Cadence |
| Withdrawal Management (Detox) | Per-diem | H0010, H0011, H0012, H0014 | Daily nursing + physician notes |
| Residential Treatment | Per-diem | H0017, H0018, H0019 | Daily clinical + group notes |
| Partial Hospitalization (PHP) | Per-diem or per-encounter | H0035, S0201 | Per-encounter notes + group attendance |
| Intensive Outpatient (IOP) | Per-encounter | H0015, S9480 | Per-encounter notes + group attendance |
| Outpatient Therapy | Per-session | 90791, 90834, 90837, 90847 | Per-session notes |
| Medication-Assisted Treatment | Bundled or unbundled | H0020, H0033, J-codes (methadone, buprenorphine) | Per-administration + counseling notes |
| Telehealth (any LOC) | Service code + modifier | Underlying code + 95 or GT modifier; POS 02 or 10 | Per-encounter notes |
Group therapy EHR billing is sensitive to attendance documentation. Payers may down-code or deny if the count, duration, or facilitator credentials are not visible in the note.
MAT is increasingly subject to bundled payment in some Medicaid plans, which changes how methadone administration and counseling are submitted.
Telehealth modifiers (95 versus GT) and place-of-service codes (02 versus 10) shifted again in 2024–2025. Verify your current payer instructions rather than relying on prior workflows.
State Medicaid plans add another layer. Managed Medicaid plans, regional managed care organizations (MCOs), and Medicaid waiver programs each carry their own auth requirements and rate sheets. Behavioral health programs that grew across states almost always run a payer rules library that captures these variations rather than relying on tribal knowledge.
Must-Have Features in Modern EHR Billing Software
Modern EHR billing software needs functional depth across intake, claims, denials, patient payments, and reporting, not a single dashboard that is glossy on the demo and brittle in production. The features below are the ones experienced behavioral health billing leads test for when evaluating an EHR platform.
Intake and front-end. Real-time eligibility, automated charge capture, configurable fee schedules, prior-authorization tracking, and verification of benefits workflows with single-case agreement support.
Claims. Payer-specific rule libraries, multi-level claim scrubbing, clearinghouse access, both UB-04 and CMS-1500 support, AI-assisted coding suggestions with confidence levels and human edit paths, and split-billing logic for group sessions.
Denials. Reason-code classification, automated routing by denial type, templated and AI-drafted appeals, immutable audit logs, and denial-pattern reporting that shows where rule tuning is needed.
Patient payments and reporting. Electronic remittance (835) auto-posting, online statements, card-on-file, payment plans, multi-location accounts receivable (A/R) dashboards, and denial-trend reporting segmented by payer and clinician.
Vendor evaluation questions to ask:
- How are payer rules configured and updated?
- Are AI coding suggestions auditable and editable?
- Which clearinghouses and remittance formats are supported?
- Can we see a live walkthrough of a denial-appeal workflow with audit logs visible?
The answer quality predicts production reliability. See the top features to look for in a behavioral health EMR for additional evaluation criteria.
How Integration Reduces Claim Denials
Integration cuts predictable denials because the rules that cause claim rejections, eligibility, coverage, modifier logic, place-of-service, documentation level, are enforced at the encounter rather than after submission. A standalone billing system can scrub claims, but it cannot prevent a clinician from documenting a level of care the patient’s plan does not cover. A connected EHR can.
Real-time edits and payer rules. Front-end edits catch formatting and logic errors at the documentation layer. Payer rule libraries apply insurer-specific constraints before submission so claims align with coverage requirements.
Automated charge capture and coding. Mapping clinical entries to CPT, HCPCS, and ICD-10 reduces miscoding and missing charges. AI-assisted coding can speed routine work, though human review remains essential for complex cases.
Layered claim scrubbing. Multi-level scrubbing runs format checks, clinical-logic validation, and payer-specific edits as an automated process. This raises first-pass acceptance and shortens the rework queue for denied claims.
Denial workflows. Automated routing, reason-code classification, and templated appeals speed resolution and surface repeat denial patterns you can address in upstream documentation or rule libraries.
A built-in billing module inside the EHR is designed to support these gains, but the actual denial-rate improvement depends on payer rule maintenance, staff training, and the discipline of weekly KPI review.
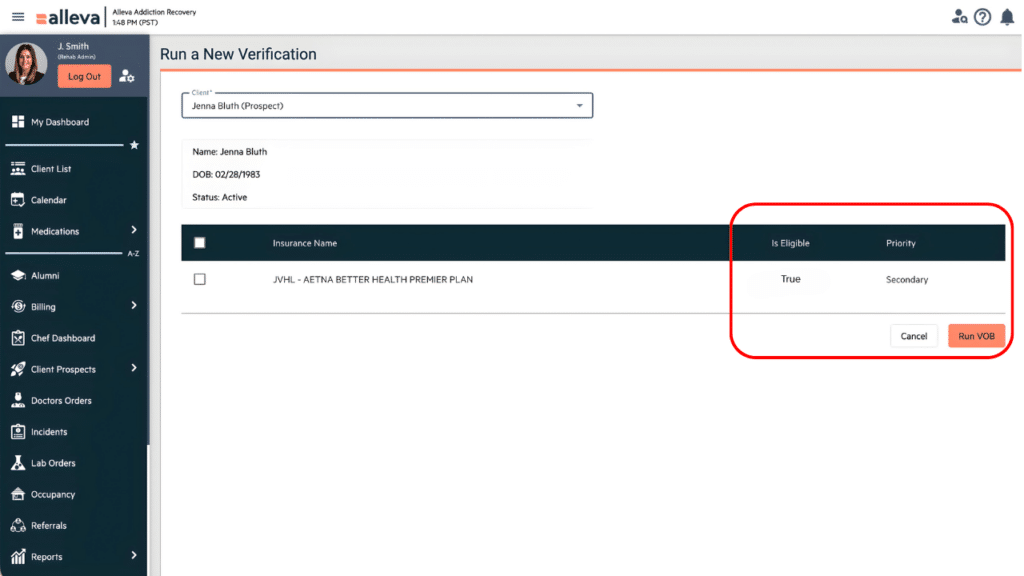
EHR Billing Real-Time Eligibility and Verification of Benefits
Real-time eligibility checks query payers using HIPAA 270/271 transactions or payer APIs and return coverage, plan type, deductible balance, copay, and prior-authorization flags within seconds. For behavioral health intake, that snapshot is the difference between confirmed coverage at booking and a surprise self-pay balance after admission.
Behavioral health VOB is more involved than primary care eligibility. Programs commonly verify level-of-care benefits, session limits, prior-authorization requirements, single-case agreement options, and telehealth coverage at the program’s licensure level.
A streamlined VOB process typically pairs an automated eligibility query with a structured payer call script for items the APIs do not return.
Eligibility queries can fail when payers lack online endpoints, return stale data, or require separate prior-authorization workflows. Behavioral health insurance company plans also tend to bundle services in ways that simple coverage flags do not capture.
Train front-desk staff to run eligibility at booking and again at check-in, save the benefit snapshot in the chart, and reserve hold slots for any case that needs authorization before service.
AI-Powered Prior Authorization and Automated Appeals, The 2024–2026 Shift
The frontier of behavioral health revenue cycle right now is automation of prior authorization and denial appeals, administrative tasks that have historically consumed enormous staff capacity. Two converging developments, often packaged under vendor names like AI Assist or similar, are reshaping how this work gets done.
Electronic prior authorization (ePA) using HL7 DaVinci PAS
The HL7 DaVinci Project’s Prior Authorization Support (PAS) implementation guide defines a FHIR-based workflow for submitting prior-auth requests electronically and receiving responses in near-real-time.
CMS rules finalized in 2024 require many payers to support electronic prior authorization APIs by 2027, with significant adoption already underway. For behavioral health, this matters because PHP, IOP, and residential admissions almost always require prior authorization, and the manual fax-and-call workflow is the largest single source of admission delays.
RPA for claims status and authorization checks
Robotic process automation (RPA) bots now log into payer portals to pull claim status and authorization expirations on a schedule, then write the results back into the EHR. This replaces the daily manual portal-checking work that EHR billing staff have done for years.
Generative-AI appeal drafting
Generative AI can read a denial reason code, pull the relevant clinical documentation from the chart, and draft a first-pass appeal letter that cites medical-necessity criteria. A human reviewer edits and signs.
Programs running this workflow report meaningfully shorter appeal cycle times, though results vary by denial type and documentation quality.
Denial-pattern clustering
Machine learning models can group denials by clinical pattern, payer, and clinician. That surfaces systemic causes (a documentation template missing a required field, a payer rule that changed last quarter) rather than treating each denial as a one-off.
Practical evaluation questions for AI features
Ask vendors a few specific things before you weigh AI capability claims:
- Are AI features auditable and editable?
- How is the model updated against payer rule changes?
- Does ePA support follow HL7 DaVinci PAS?
- Do appeal-drafting outputs preserve clinical author attribution?
Alleva’s perspective on the role of AI in behavioral health frames AI as a layer that supports clinical and EHR billing teams rather than replacing judgment.
The honest caveat: AI in revenue cycle is moving faster than most payers’ acceptance criteria. Treat early-stage AI features as productivity accelerants, keep humans in the loop on every claim and appeal, and tune as you go.
How Integration Speeds Submission and Reimbursement
Integrating a behavioral health EHR billing reduces manual handoffs and accelerates cash flow. The mechanism is simple: data captured at the encounter flows into claim assembly without re-keying, and the gaps that delay submission shrink.
The typical workflow runs through six steps:
- Capture structured intake and visit data at the encounter so required fields are complete.
- Map clinical elements to CPT and ICD codes automatically.
- Run pre-submit scrubbing against payer rules.
- File claims electronically as encounters close.
- Auto-post EOBs and trigger appeals or patient billing.
- Monitor A/R metrics weekly.
Implementation rigor matters more than feature count. The steps that move the needle are familiar:
- Standardize visit templates.
- Enable coding automation cautiously.
- Configure payer rules.
- Train staff.
- Monitor weekly.
Programs that follow this discipline tend to see measurable improvement in days in A/R within the first two quarters after go-live, though specific gains depend on starting state and payer mix.
Reporting, Analytics, and KPIs to Track
Reporting and analytics turn EHR billing performance from anecdote into decision-grade data. A focused KPI dashboard surfaces cash velocity, leakage, and the few process changes that move the needle.
Core RCM KPIs for Behavioral Health: Reference Chart
| KPI | Target Range | What It Signals |
| Clean-claim rate | 90–95%+ | Front-end documentation and coding quality |
| First-pass acceptance | 95%+ | Scrubbing effectiveness and rule library accuracy |
| Days in accounts receivable (A/R) | Under 40 days | Cash velocity and follow-up rigor |
| Denial rate | Under 5–7% | Documentation, eligibility, and rule alignment |
| Net collection rate | 95%+ | Payer-mix accuracy and write-off discipline |
| Time-to-payment | Under 30 days from submission | End-to-end workflow efficiency |
| Admission-to-billing lag | Under 48–72 hours | Front-end intake-to-claim handoff |
| Authorization expiration rate | Under 2% | Prior-auth tracking and recertification cadence |
Targets are general behavioral health benchmarks and should be adjusted to your payer mix, level-of-care portfolio, and program maturity. Verify against your own historical data before setting team goals.
Behavioral health programs benefit from segmenting these KPIs by clinician, level of care, and payer. Group-session revenue, authorization expirations, copay capture, and admissions-to-billing lag reveal operational patterns that aggregate dashboards mask.
Trend, cohort, and payer-mix reports help you spot persistent leakage and prioritize fixes with measurable impact.
Patient Billing, Statements, and Good Faith Estimates
Patient-facing billing should combine portals, online statements, card-on-file, automated payment plans, copay collection at check-in, and Good Faith Estimates (GFEs) for self-pay or uninsured patients. The CMS Good Faith Estimates resource explains the No Surprises Act requirement to provide GFEs to uninsured and self-pay patients.
A clear billing experience tends to improve the overall patient experience without adding friction to patient care.
Patient portals reduce inbound calls by giving patients self-service visibility into balances, statements, and payment history. Online payments (card-on-file, ACH, recurring plans, automatic retries) accelerate collections when consent and payment-token storage are documented in your HIPAA-compliant EHR billing policies.
Behavioral health adds a privacy layer most non-BH systems do not handle well. Patients in SUD or mental health treatment may not want EHR billing communications visible to family members, and 42 CFR Part 2 imposes specific consent requirements for SUD records.
Use discreet messaging, opt-in reminders, and minimize electronic protected health information (ePHI) in notifications. Alleva’s perspective on privacy in behavioral health EMR systems covers the operational implications in more depth.
HIPAA, Security, and Audit-Readiness
EHR billing systems handle ePHI, which means HIPAA technical safeguards are non-negotiable. Strong security and privacy controls reduce breach exposure and lower legal risk.
The HHS Office for Civil Rights HIPAA enforcement guidance explains the enforcement framework for covered entities and business associates.
HIPAA-compliant hosting. PHI should sit in segregated environments with executed Business Associate Agreements (BAAs) that make legal responsibilities and access boundaries explicit.
Encryption and access controls. Data should be encrypted in transit and at rest. Role-based access plus immutable audit logs document who accessed or changed clinical and billing fields and when.
Independent attestations. SOC 2 Type II or ISO 27001 reports add external assurance, though they do not replace HIPAA compliance. They make procurement and audit conversations faster.
For programs preparing for accreditation surveys (Joint Commission, CARF) or payer audits, audit-readiness is as much about documentation discipline as it is about technology. Programs that maintain ongoing audit-ready documentation, rather than scrambling before a survey, find the process meaningfully less disruptive.
Alleva’s guide to audit-ready compliance documentation walks through the operational habits that make this possible.
Scaling From Solo Practice to Multi-Site Group
Scalability needs differ across program sizes. Solo and small practices prioritize simplicity and short time-to-value. Multi-site organizations require centralized governance, multi-entity reporting, single sign-on (SSO), and stronger access controls.
The core tradeoff is speed versus control. Solo practices move quickly with single-entity setups and weeks-long implementations. Enterprise behavioral health groups trade speed for centralized controls and richer reporting, with implementations often running three to nine months depending on payer count and legacy data complexity.
Vendor questions to test scalability fit:
- Does the system support both centralized and decentralized billing workflows?
- Can provider rosters and credentialing data sync across entities automatically?
- Is multi-entity financial reporting built in, or does it require external BI?
- What SSO and permissioning options exist?
- How are payer credentialing workflows handled at scale?
Answer quality on these points predicts whether the platform will reduce manual reconciliation work or simply shift it.
Integration Standards: HL7, FHIR, X12, and APIs
Behavioral health EHRs and billing platforms exchange data using a stack of established Healthcare IT standards: HL7 v2 for clinical event messages, FHIR for modern clinical and eligibility exchanges, X12 837 for claims and X12 835 for remittance, RESTful APIs and vendor SDKs for custom integrations, and clearinghouse links for batch claim routing.
These same standards govern how an EHR exchanges data with practice management software when the two functions live in separate systems.
Alleva’s integration with CollaborateMD is an example of how an integrated billing layer can sit alongside the clinical EHR without forcing duplicate data entry.
The same standards stack handles structured clinical artifacts beyond progress notes, intake assessments, treatment plans, lab results, and even radiology reports referenced from external imaging systems. Behavioral health programs that touch primary care or refer out for medical workups can receive results inside the same medical record.
Several practical disciplines separate integrations that hold together from integrations that fail at go-live:
- Validate payloads, error handling, and authentication in payer sandboxes before production cutover.
- Map CPT, ICD-10, HCPCS, and NDC code sets explicitly to your billing rules.
- Run end-to-end payer simulations covering eligibility, claim submission, and remittance reconciliation.
- Test behavioral-health-specific fields and modifiers (group attendance, MAT administration, telehealth POS).
Integration testing typically runs four to eight weeks. Go-live validation runs another one to two weeks, longer for complex payer mixes. Plan for phased cutovers, keep clinicians and billers in the loop, and publish rollback procedures before the first claim crosses.
Common Integration Challenges and How to Mitigate Them
Integration challenges in behavioral health revenue cycle cluster around data migration, payer rule drift, and staff workflow alignment. Each has a known mitigation pattern.
Data migration and code mapping
Incorrect code mapping inflates denial rates after cutover. Validate mappings in sandboxes, run parallel billing during the transition window, and reconcile legacy code translations before closing the gap.
Dual-run billing catches mismatches without stopping cash flow.
Payer rule drift
Payer rules change continually, causing rule libraries to fall out of date and producing predictable rejections. Vendors mitigate this with rule engines that update on a schedule (often weekly or event-driven), governed by service-level agreements (SLAs).
Confirm the cadence, the escalation path for emergency edits, and who owns rule maintenance during onboarding and steady state.
Staff training and workflow validation
Documented workflows almost always differ from real workflows. Combine role-based training, scenario-based exercises, and end-to-end testing with the people who actually run the work, medical billers, intake staff, and healthcare providers across each level of care.
Short, role-specific go-live checklists outperform long generic training decks.
Vendor consolidation risk
The behavioral health EHR market has consolidated meaningfully in 2023–2026. Operators who chose vendors that were later acquired or sunset have absorbed real switching costs.
The hidden cost of EMR vendor consolidation covers what to verify about a vendor’s roadmap, ownership, and investment commitment before signing.
A clean go-live checklist usually splits responsibilities. Vendor: sandbox environment, test plans, SLA, rollback plan. Internal: data cleanup, dual-run sign-off, staff training completion, week-one daily standups.
Single-Vendor Integrated EHR vs. Best-of-Breed RCM
The choice between an integrated EHR + RCM platform and a best-of-breed pairing affects revenue performance, audit prep, and total cost of ownership. Both models can work, what matters is matching the model to your operational reality.
Integrated systems share a single data model. That lowers manual reconciliation, shortens audit prep, and reduces training surface area. Best-of-breed RCM, paired with a separate EHR via interfaces, can offer deeper denial-management capabilities and faster payer-rule responsiveness, at the cost of interface maintenance and reconciliation work.
A practical decision framework weighs four factors:
- Organization size and multi-location complexity. Smaller programs benefit disproportionately from a single platform.
- Case mix and billing complexity. Programs with heavy out-of-network work or high-volume appeals may benefit from specialized RCM depth.
- In-house billing expertise and vendor management capacity. Best-of-breed assumes someone owns the interface and the SLA.
- Growth plans and vendor lock-in tolerance. Multi-state expansion changes the math toward integrated platforms.
Score these against integration tightness, feature depth, flexibility, and vendor risk to clarify which model fits your operational priorities.
Data Ownership, Exportability, SLAs, and Uptime
Data ownership determines who controls PHI when the relationship ends. Contractual and technical controls need to align with regulatory responsibility, and HHS OCR guidance confirms that covered entities remain responsible for their business associates regardless of vendor performance.
Contract clauses to insist on.
- Customer retains ownership of clinical and billing data; vendor signs a BAA.
- Export formats include CSV and HL7/FHIR for clinical data and X12 for billing data.
- Backup and restore obligations include routine restore tests, not just backup runs.
- Encryption at rest and in transit is documented with specific algorithms.
- Recovery time objective (RTO) and recovery point objective (RPO) are defined with measurable targets.
- Uptime targets carry service credits, and historical uptime is published.
- Incident response timelines and escalation paths are explicit.
Vendor demo questions to ask:
- Can you show sample export files and a tested restore?
- What is your published uptime, and where is it posted?
- Do you perform daily backups?
- Will you sign a BAA with export rights named in the contract?
- Can we see your incident response runbook?
Procurement targets. Common targets (RTO of four hours or less, RPO of one hour or less, 99.9% uptime with service credits) are reasonable starting points but should be adjusted to your operational risk tolerance and verified with your legal and IT teams.
How Operational Software Supports Behavioral Health Billing
Behavioral health operations software encodes payer rules, accreditation evidence, and grouped-charge logic into configurable workflows. That layer of behavioral-health-specific configuration is what separates platforms that ship clean claims from generic healthcare systems adapted after the fact.
Behavioral-health platforms typically handle admission bands, group-therapy split logic, MAT codes, multi-payer adjudication with state-specific rules, accreditation-ready documentation, and audit trails as first-class features rather than custom configurations. Integrated scheduling, prior-authorization tracking, and real-time clinical notes keep billing and clinical records aligned to reduce denials and rework.
Operational dashboards connect claims outcomes to KPIs so leaders can see revenue leakage and prioritize fixes. The combination of behavioral-health-specific workflows and an integrated billing layer is designed to match the complexity of behavioral health programs without forcing your team to maintain workarounds.
See Integrated EHR Billing in Action
Behavioral health revenue cycle is detail work, payer rules, level-of-care logic, group-session attendance, prior authorization, denial appeals. The platform you choose either absorbs that complexity or hands it back to your staff every day.
If you are evaluating whether an integrated EHR and RCM platform built for behavioral health fits your program, request a demo of Alleva and we will walk through the workflows that match your level-of-care mix and payer set.
EHR Billing Frequently Asked Questions
Here are some questions people also ask about EHR billing, software integrations, and medical billing for behavioral health more generally.
What is EHR billing and how does it differ from standalone medical billing software?
EHR billing combines clinical documentation and revenue cycle so charges flow from notes and encounter records into claim assembly, coding, scrubbing, and submission. The flow supports CMS-1500 and UB-04 claims and uses X12 837 for submission and X12 835 for remittance.
Standalone systems require manual or interface-driven imports of clinical data, which adds duplicate entry and reconciliation work.
Will integrating my EHR with billing software actually reduce claim denials?
Integration cuts predictable denials when front-end edits, payer-specific rules, and eligibility checks fire at the point of care. The biggest gains come from consistent charge capture and pre-submit scrubbing, though results depend on rule-library maintenance, governance, and staff training.
Expect denial volumes to fall gradually as rules tune to your payer mix and as denial-management workflows address repeat patterns.
How accurate is AI-assisted coding, and can we trust it?
AI-assisted coding analyzes clinical notes and suggests CPT, HCPCS, and ICD-10 codes with confidence levels. Accuracy varies by specialty, documentation quality, and how the model has been trained. Use AI suggestions as a productivity layer that reduces routine errors while keeping clinician and certified coder review for complex claims and payer-specific edge cases.
Does an integrated system support real-time insurance eligibility verification?
Most modern integrated systems connect to payer eligibility services and return coverage, plan type, active benefits, and prior-authorization flags at scheduling or check-in. Real-time checks can fail when payer systems are down, subscriber data is incomplete, or coverage changed recently, so front-desk workflows should include a quick verification step and a fallback confirmation method.
How long does an EHR-to-billing integration typically take?
Single-practice integrations commonly complete in several weeks to a few months. Phases include discovery and mapping, configuration and rule-building, sandbox testing, parallel pilot, and full cutover with monitoring. Multi-site or multi-state programs often run three to nine months due to payer count, custom code sets, and legacy data migration complexity.
What KPIs should we track after implementation?
Track clean-claim rate, first-pass acceptance, days in A/R, denial rate, net collection rate, and time-to-payment. For behavioral health, add admission-to-billing lag, group-session revenue by clinician, authorization expiration rate, and copay capture at check-in. Use these to identify revenue leakage, validate rule tuning, and measure productivity improvement.
Who owns the clinical and billing data, and how do we export it if we switch vendors?
Contracts should state explicitly that the customer retains ownership and that the vendor provides export procedures. Confirm export formats (CSV, HL7, FHIR, X12, database extracts), timeframe, and any fees. Include a clause requiring a full data extract and a tested restore during procurement so portability is validated rather than assumed.
Does the system support UB-04 facility billing and multi-location centralized billing?
Mature platforms support both UB-04 institutional and CMS-1500 professional claims, multi-location payer credentialing, and centralized work queues for a single revenue team across multiple sites. Confirm support for facility-level charge masters, consolidated statements, consolidated 835 posting, and role-based permissioning before signing.
What is electronic prior authorization (ePA), and why does it matter now?
Electronic prior authorization uses FHIR-based standards (most often the HL7 DaVinci PAS implementation guide) to submit prior-auth requests without fax or phone calls. CMS rules require many payers to support ePA APIs by 2027, and behavioral health admissions almost always require prior authorization. Faster ePA cycles reduce admission delays.